18 September 2025
DEP irinotecan boosts immuno-oncology in colon cancer models
- DEP® irinotecan in combination with an immuno-oncology (IO) therapy (anti PD-1 antibody) resulted in superior anti-tumour activity and significant survival benefit compared to the IO therapy alone in two colorectal cancer (CRC) models
- This combination benefit did not occur when conventional irinotecan was used together with the same IO therapy (anti-PD1 antibody)
- IO agents are now important treatments in several major cancers and the market for these agents is expected to exceed US$55 billion by 2025[1], and include Merck’s Keytruda®, BMS’ Yervoy® and AstraZeneca’s Imfinzi®
- Starpharma’s proprietary SN-38 nanoparticle, DEP® irinotecan is currently in phase 2 and these data in the CRC models provide important information which will assist with the identification of value-adding clinical combinations and partnering opportunities
Melbourne, Australia; 29 June 2020: Starpharma (ASX: SPL, OTCQX: SPHRY) today announced its SN-38 nanoparticle, DEP® irinotecan in combination with an immuno-oncology (IO) agent (anti PD-1 antibody) showed superior anti-tumour activity and significant survival benefit in two colorectal cancer (CRC) models when compared to the anti PD-1 antibody alone. These results included improvement in both survival and efficacy in the particularly aggressive CT-26 CRC model.
The median survival for the combination of DEP® irinotecan + IO agent (anti PD-1 antibody) was 40 days compared with 13 days for the IO agent alone (refer to the study results below). The enhanced combination benefit seen with DEP® irinotecan was not seen with conventional irinotecan + the same IO agent. These preclinical results provide a strong rationale for clinical evaluation of DEP® irinotecan in combination with IO agents, potentially opening up significant additional commercial opportunities.
IO agents including Keytruda® (an anti PD-1 antibody) have been approved and have been highly successful in a range of cancers including lung cancers and melanoma. However clinical trial results thus far with IO agents alone have been disappointing in some cancers, including CRC. Anti PD-1 antibodies have been a major breakthrough in cancer treatment, but substantial unmet need remains and non-responders make up more than 75% of all incident cancers, highlighting the need for more effective agents and combinations[2].
DEP® irinotecan is a novel, patented dendrimer nanoparticle of SN-38, the active metabolite of irinotecan. DEP® irinotecan recently progressed to phase 2. In a phase 1 trial conducted in major cancer centres in the UK, DEP® irinotecan was well-tolerated and patients generally experienced less severe side effects than with conventional irinotecan, including no cases of severe diarrhoea, for which conventional irinotecan has a FDA black box warning. Encouraging efficacy signals with DEP® irinotecan were also observed in 50% of evaluable patients - not only in patients with CRC but also in patients with breast and pancreatic cancer.
Dr Jackie Fairley, Starpharma CEO, commented: “We are delighted to see the dual benefits of combining DEP® irinotecan with an immuno-oncology (IO) agent. These results indicate that DEP® irinotecan in combination with an anti PD-1 antibody could boost the efficacy over anti PD-1 antibody alone, or IO combinations with standard chemotherapeutic agents. IO agents including anti PD-1 antibodies have yielded excellent efficacy results in some patient groups. However, between 30-60% of patients do not respond to IO treatments alone[3], therefore there is significant commercial interest in combination approaches, including with chemotherapeutics, to overcome this limitation[4]”.
“In addition, there have been no observations of immune-mediated toxicities in patients treated with DEP® irinotecan. Given immune-mediated toxicities can be problematic with IO agents, the lack of overlapping side-effects further strengthens the rationale for combining IO agents with DEP® irinotecan”, added Dr Fairley.
DEP® irinotecan is one of three DEP® products in clinical development by Starpharma, and is currently in a phase 2 clinical trial at leading UK hospitals, The Christie, The Royal Marsden and Newcastle Freeman Hospital. Two further sites, the Beatson (Scotland) and Kinghorn Cancer Centre (Sydney) will be opened shortly.
The market for IO agents is expected to exceed US$55 billion by 2025[5]. Market leading products include the PD-1 antibody Keytruda (Merck; 2019 sales: US$ 11.08B)[6] and Opdivo (BMS; 2019 sales: US$ 7.20B), the CTLA-4 inhibitor Yervoy (BMS; 2019 sales: US$ 1.49B)[7] and the PD-L1 inhibitor Imfinzi (AZ; 2019 sales: US$ 1.47B)[8].
Study Results
Significant enhancement of anti PD-1 antibody (anti PD-1 Ab) activity by DEP® irinotecan in both CT-26 and MC-38 colon cancer models (Figure 1 and 2)
Anti PD-1 antibody alone had minimal impact on this CT-26 model, but efficacy was greatly enhanced when combined with DEP® irinotecan in both the CT-26 (Figure 1) and MC-38 (Figure 2) models. The CT-26 model is recognised as being a highly aggressive CRC model, therefore this result is particularly impressive.
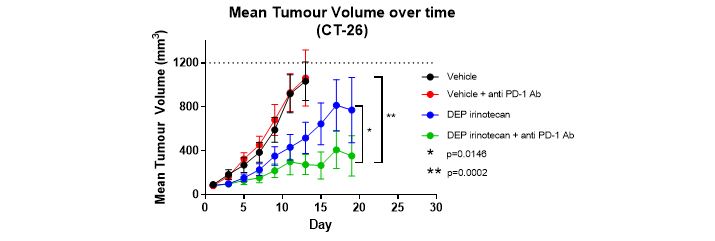
Figure 1: Mean tumour volumes over time as measured in the mouse allograft study using CT-26 murine colorectal cancer cells (n=5). DEP® irinotecan + anti PD-1 Ab in combination had a statistically significant greater anti-tumour effect than anti PD-1 Ab alone (p=0.0002) and DEP® irinotecan alone (p=0.0146).
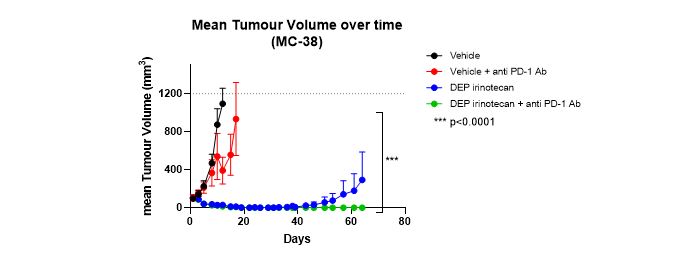
Figure 2: Mean tumour volumes over time as measured in the mouse allograft study using MC-38 murine CRC cells (n=5). DEP® irinotecan + anti PD-1 Ab combination had a statistically significant greater anti-tumour effect compared with anti PD-1 Ab alone (p=0.0001).
Significant survival benefit seen with DEP® irinotecan + anti PD-1 Ab combination (Figure 3)
Enhanced survival, which was statistically significant, was seen in both the DEP® irinotecan treated group and the DEP® irinotecan + anti PD-1 Ab combination group (Figure 3a CT-26 (p=0.0014) and Figure 3b MC-38 (p<0.0001)). Median survival was extended more than 3‑fold, from 13 days (anti PD-1 Ab alone) to 40 days (DEP® irinotecan + anti PD-1 Ab) in the CT-26 allograft study and 22 days (anti PD-1 Ab alone) to >64 days (DEP® irinotecan + anti PD-1 Ab) in the MC-38 allograft study.
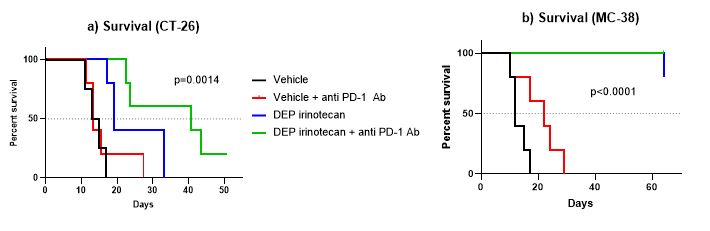
Figure 3: Kaplan-Meier survival curve in the mouse allograft study using a) CT-26 and b) MC-38 murine CRC cells. Dotted line shows the median survival (days).
Superior combination benefit of anti PD-1 Ab provided by DEP® irinotecan compared to conventional irinotecan
The combination of DEP® irinotecan + anti PD-1 Ab had a significantly greater anti-cancer effect than anti PD-1 Ab alone (p=0.0016) or conventional irinotecan + anti PD-1 Ab (p=0.0156) and the DEP® irinotecan + anti PD-1 Ab combination also showed improved survival (p<0.0001). Median survival was extended from 14 days (anti PD-1 Ab alone) to 27 days (DEP® irinotecan + anti PD-1 Ab) in the CT-26 model.
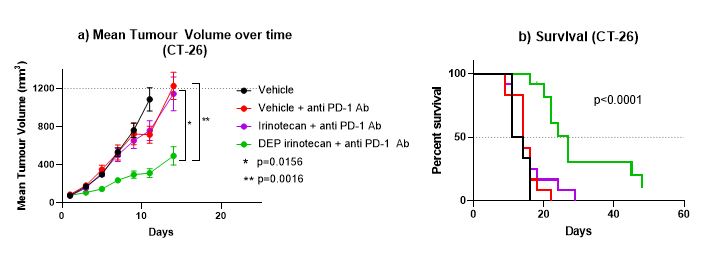
Figure 4:
a) Mean Tumour volumes over time as measured in the mouse allograft study using CT-26 murine colorectal cancer cells (n=12);b) Kaplan-Meier survival curve in the mouse allograft study using CT-26 murine colorectal cancer cells. Dotted line shows the median survival (days).
Study Methods
These studies were conducted for Starpharma by an internationally recognised translational cancer group using mouse allograft models which are the standard means of assessing efficacy of IO agents, including anti PD-1 antibodies. Testing of IO agents requires a functioning immune system, so anti-cancer efficacy cannot be assessed in human cancer xenograft models.
Study 1:
Balb/c mice were inoculated subcutaneously with the murine colorectal (CT-26) cell line (5 mice/group). Dosing groups were as follows:
- Vehicle Control: - antibody isotype control, twice weekly ip, for 4 doses - on day 1 (200 µg per mouse) then on days 5, 8 and 12 (100 µg per mouse)
- Anti PD-1 Ab: anti PD-1 Ab, twice weekly ip, for 4 doses - on day 1 (200 µg per mouse) then on days 5, 8 and 12 (100 µg per mouse)
- DEP® irinotecan: DEP® irinotecan (18mg/kg) once weekly iv, for 3 weeks and antibody isotype control twice weekly ip, for 4 doses
- DEP® irinotecan + anti PD-1 Ab: DEP® irinotecan once weekly iv, for 3 weeks and anti PD-1 antibody twice weekly ip, for 4 doses
Study 2:
C57BL/6 mice were inoculated subcutaneously with murine colorectal (MC-38) cells (5 mice/group). Dosing groups were as follows:
- Vehicle Control: - antibody isotype control, twice weekly ip, for 4 doses - on days 1, 5, 8 and 12 (200 µg per mouse)
- Anti PD-1 Ab: anti PD-1 antibody, twice weekly ip, for 4 doses - on days 1, 5, 8 and 12 (200 µg per mouse)
- DEP® irinotecan: DEP® irinotecan (30mg/kg) once weekly iv, for 3 weeks and antibody isotype control twice weekly ip, for 4 doses
- DEP® irinotecan + anti PD-1 Ab: DEP® irinotecan (30mg/kg) once weekly iv, for 3 weeks and anti PD-1 antibody twice weekly ip, for 4 doses
Study 3:
Balb/c mice were inoculated subcutaneously with murine colorectal (CT-26) cells (12 mice/group). Dosing groups were as follows:
- Vehicle Control: - antibody isotype control, twice weekly ip, for 4 doses - on day 1 (200 µg per mouse) then on days 5, 8 and 12 (100 µg per mouse)
- Anti PD-1 Ab: anti PD-1 Ab, twice weekly ip, for 4 doses - on day 1 (200 µg per mouse) then on days 5, 8 and 12 (100 µg per mouse)
- Irinotecan + anti PD-1 Ab: Irinotecan (75mg/kg) once weekly iv, for 3 weeks and anti PD-1 antibody twice weekly ip, for 4 doses
- DEP® irinotecan + anti PD-1 Ab: DEP® irinotecan (20mg/kg) once weekly iv, for 3 weeks and anti PD-1 Ab twice weekly ip, for 4 doses
In all studies, tumours were measured twice weekly using electronic callipers. The tumour volume (mm3) data represent the mean ± standard error of the mean (SEM). Tumour volume data was analysed using a two-way ANOVA - mixed effects analysis. Survival curves were analysed using ANOVA with a Log-rank (Mantel-Cox) test. Note: If error bars do not display on the graphs, they are not visible because they are shorter than the height of the symbol.
Download ASX Announcement: DEP® irinotecan boosts immuno-oncology in colon cancer models (PDF, 112kb)
[1] https://www.alliedmarketresearch.com/immune-check-point-inhibitors-market
[2] August 2019 IO presentation by Peter F Lebowitz (M.D. PhD), Global Therapeutic Area Head, Oncology, Janssen Oncology, with data sourced from Cancer Incidence from Globocan 2018.
[3] Mengjia Song, Xinfeng Chen, Liping Wang, and Yi Zhang, 2018. Future of anti PD-1/PD-L1 applications: Combinations with other therapeutic regimens, Chin J Cancer Res. Apr; 30(2): 157–172
[4] Le, C.T., Murphy, W.J. Moving forward to address key unanswered questions on targeting PD-1/PD-L1 in cancer: limitations in preclinical models and the need to incorporate human modifying factors. j. immunotherapy cancer 7, 291 (2019).
[5] https://www.alliedmarketresearch.com/immune-check-point-inhibitors-market
[6] https://www.mrknewsroom.com/news-release/corporate-news/merck-announces-fourth-quarter-and-full-year-2019-financial-results
[7] https://news.bms.com/press-release/corporatefinancial-news/bristol-myers-squibb-reports-fourth-quarter-and-full-year-fi-1
[8] https://www.astrazeneca.com/content/dam/az/PDF/2019/full-year/Full-year_and_Q4_2019_results_announcement.pdf